- Mary O'Hara
- The Observer, Sunday 19 April 2009
- Article history
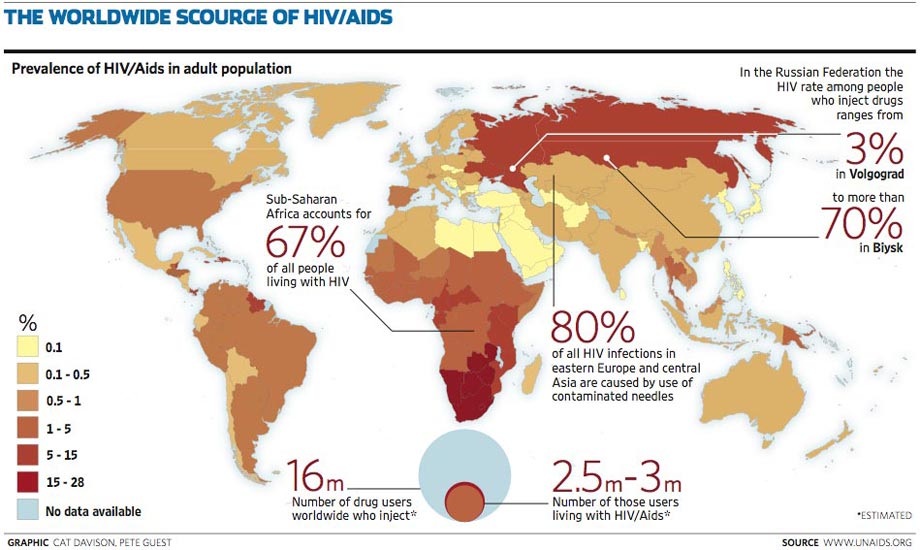
Aids and HIV worldwide. Photograph: Cat Davison/Pete Guest
The use of illicit drugs must be decriminalised if efforts to halt the spread of Aids are to succeed, one of the world's leading independent authorities on the disease has warned.
In an unprecedented attack on global drugs policy, Michele Kazatchkine, head of the influential Global Fund to Fight Aids, Tuberculosis and Malaria, has told the Observer that, without a radical overhaul of laws that lead to hundreds of thousands of drug users being imprisoned or denied access to safe treatment, the millions of pounds spent on fighting HIV and Aids will be wasted.
Kazatchkine will use his keynote speech at the 20th International Harm Reduction Association conference tomorrow in Bangkok to expose the failures of policies which treat addiction as a crime. He will accuse governments of using what he calls "repressive" measures that deny addicts human rights rather than putting public health needs first.
He will argue that governments should fully commit to the widespread provision of harm reduction strategies aimed at intravenous drug users, such as free needle exchanges and providing substitutes to illicit drugs, such as methadone.
"A repressive way of dealing with drug users is a way of facilitating the spread of the [HIV/Aids] epidemic," Kazatchkine said. "If you know you will be arrested, you will not go for treatment. I say drug use cannot be criminalised. I'm talking about criminalising trafficking but not users. From a scientific perspective, I cannot understand the repressive policy perspective."
He condemns policymakers who argue that, because drug users frequently turn to crime to fund their habit, it justifies making it a criminal justice issue. Harm reduction both helps the addict and wider society and reduces the need to commit crime, he said.
"The one population where [Aids] mortality has been untouched - and in fact has worsened - has been IV [intravenous] drug users. It's amazing, because what we call harm reduction, such as exchanging needles, has been scientifically proven as the most effective.
"This is why I will most probably start my speech in Bangkok by mentioning the contrast between major progress achieved in decreasing mortality from Aids in the poorest countries of the world versus the total lack of progress for what is the main route of transmission in most parts of the world outside Africa."
Kazatchkine suggested that politicians feared that the public would label them soft on drugs. A doctor and respected Aids expert with 20 years in the field, he has in his two years at the helm of the Global Fund overseen some of the most dramatic improvements in treatment and prevention of HIV globally.
Since it was established in 2001, the fund has received $21bn in contributions from the world's wealthiest nations and used it to play a significant part in reducing rates of new HIV infections. It has also contributed to the distribution of much needed life-preserving anti-retroviral drugs to millions of people already diagnosed.
Alex Stevens, a senior research fellow specialising in drugs and criminalisation at the University of Kent, said tomorrow's speech would highlight many of the troubling consequences of criminal justice approaches to drugs policy.
"In many countries, serious human rights infringements are committed in the name of fighting drugs," he said. "These include the use of the death penalty for drug offences, compulsory treatment regimes that include methods (such as physical beatings) that are akin to torture, and, for example in the USA, depriving convicted drug law offenders of the right to vote."
Stevens said that, while the UK was ahead of many other countries on harm reduction, its tendency to criminalise drug users could undermine its efforts.
What is needed, Kazatchkine will argue tomorrow, is a total rethink of drugs policies. "What I'm saying is that government's function is to protect their citizens. This is why harm reduction should be supported by all governments everywhere."




